During accessory-breast consultations, there is one question we hear most often.
“Doctor, doesn’t this go away if you just remove the gland?”
From the outside, it can look like a bulging lump in the armpit, so it’s natural to think that way.
But in reality, accessory breast surgery is not simply about removing a lump.
To properly address accessory breast tissue, you must design thickness, skin laxity, and the silhouette together.
Accessory Breast Surgery
Not a surgery to ‘remove gland tissue,’ but a surgery to shape the silhouette
What is an accessory breast?
Its relationship to the milk line (Milk line)
An accessory breast is not simply a lump of fat.
It is a structural phenomenon related to mammary development during fetal life.
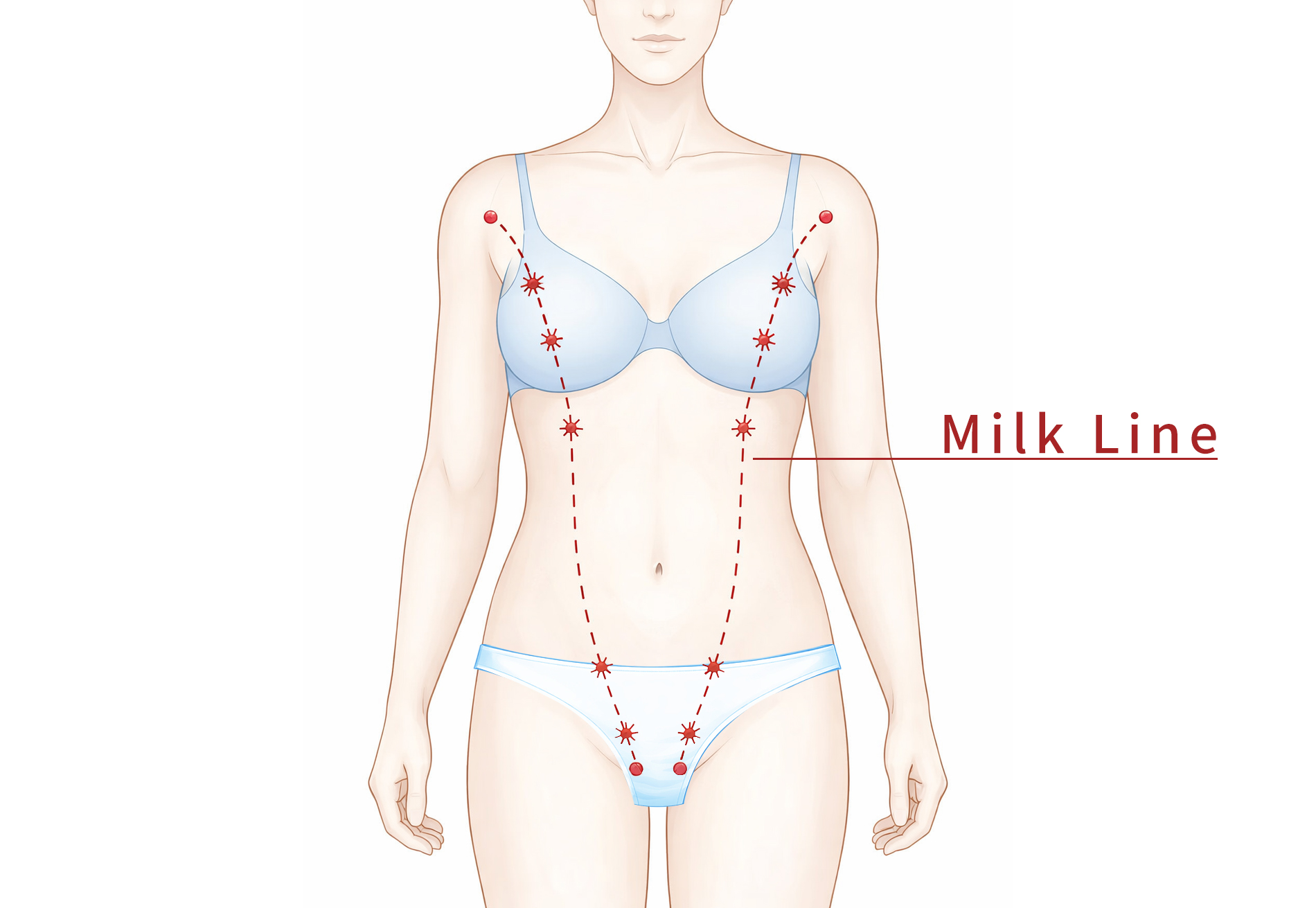
What is the milk line (Milk line)?
Around fetal weeks 4–6, a temporary line (mammary ridge) forms from the armpit to the groin where mammary glands can develop.
Normally, most of this line regresses, leaving only the breast area to form normal breasts. But if regression is incomplete, remnants of breast tissue can remain somewhere along the path.
This can lead to the following presentations.
· Accessory breast
· Accessory nipple
· Hormone-responsive lumps in the armpit, abdomen, or groin
So some people may experience situations like the following.
 Pain before menstruation
Pain before menstruation
Size increase during pregnancy/breastfeeding
Key concept of accessory breast?
A spectrum issue : not simply ‘present / absent’
Accessory breast should be understood as a difference in the degree of regression—i.e., a spectrum.
The accessory-breast spectrum includes all of the following.
· Gland + fat remaining together
· Predominantly fatty type
· Only the nipple remaining
· Nipple and gland remaining together
So the important question is this.
❌ “Is there gland tissue or not?”
⭕ “Is there glandular parenchyma that should be meaningfully removed surgically?”
Why do we need to differentiate tissue density?
There is one reason: because the surgical method changes completely.

Glandular-type Accessory Breast
· Significant glandular parenchyma remains
· Tissue may remain with liposuction alone
· Hormone-responsive pain/volume changes may persist
➡ Gland excision is needed
Fatty-type Accessory Breast
· Fat is the main component
· Only a minimal amount of gland tissue
· In many cases, liposuction alone can achieve sufficient results
➡ Liposuction-focused approach
The precise meaning of ‘fatty-type accessory breast’
Histologically, gland tissue and fat are almost always mixed.
The same is true for normal breasts.
So the expression “there is absolutely no gland tissue” is not accurate.
Clinically, “fatty-type accessory breast” means:
· Ducts/lobules are minimal
· Almost no hormonal response
· Not enough volume to justify surgical excision
This is not a diagnosis, but a clinical classification for surgical decision-making.
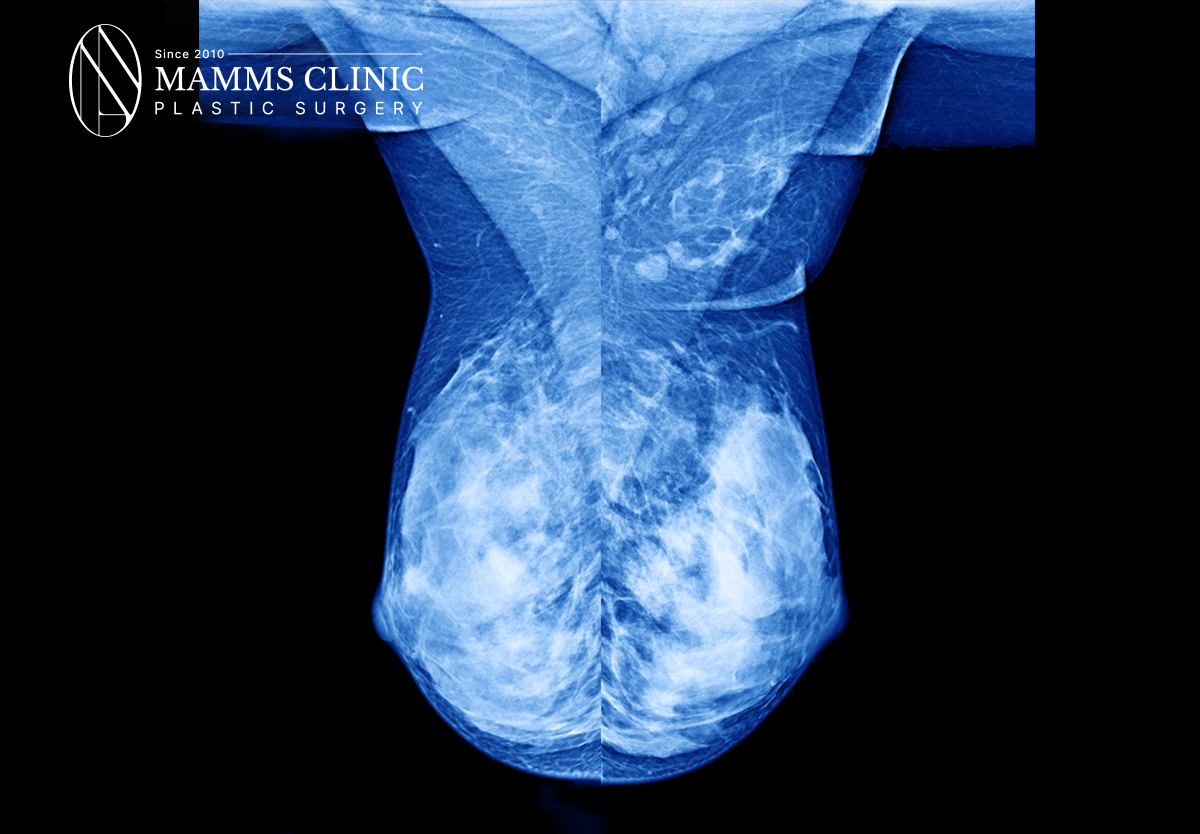
Mamms Surgical & Plastic Surgery Clinic Breast X-ray Sample
At Mamms Surgical & Plastic Surgery Clinic, we use breast X-rays to confirm ✔ tissue thickness and ✔ density, and we use these as standards for surgical design.
The essence of accessory breast surgery
Not a removal surgery, but a ‘surgery to restore form’
Accessory breast surgery is not a procedure that simply removes a lump.
The completeness of the surgery depends on whether you design these three things at the same time.
1️⃣ How to remove the internal tissue
2️⃣ What happens to skin laxity after removal
3️⃣ The final silhouette where the arm and breast connect

Why is accessory breast a three-dimensional issue?
Even if it looks like a small bulge on the surface, accessory breast tissue actually spreads three-dimensionally—from the front axillary fold, to the arm–breast boundary, to the lower outer breast.
So the goal is:
❌ Eliminating what sticks out
⭕ Recreating the curve that flows from the armpit to the breast
Actual decision-making process for accessory breast surgery
Step 1: Remove internal tissue
First, we look at the internal problem. Whether meaningful gland tissue remains or fat is the main component, the approach differs—but the goal is the same.
👉 Make it thin naturally
In the end, the key is reducing thickness so the structure adheres closely to the base.

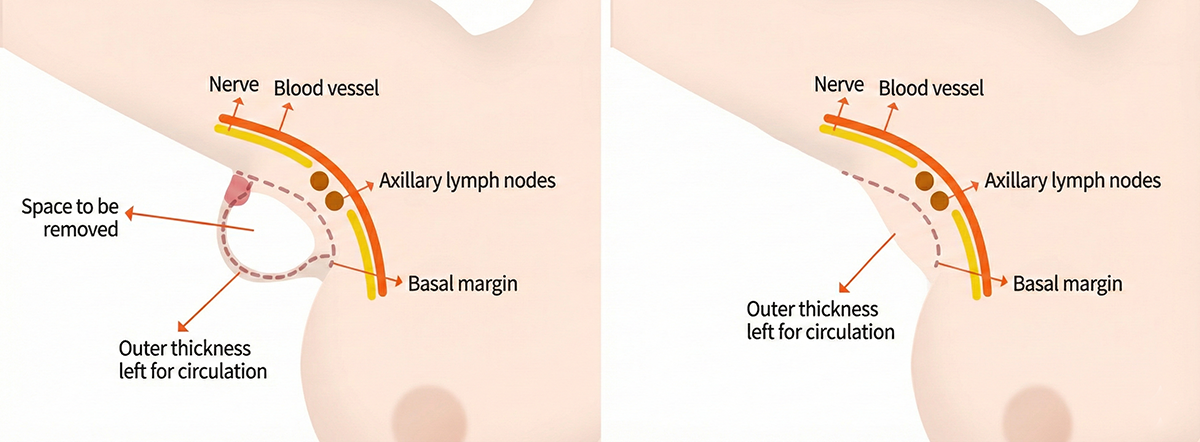
5mm Rule – a standard that must be followed
This is the most important standard I adhere to in accessory breast surgery. Skin blood flow depends on the subdermal plexus.
· Less than 5mm → decreased blood flow, risk of necrosis
· 5mm or more → safe
This number is not a cosmetic standard, but a standard for blood flow and safety.

Step 2: Bra-line contour refinement
After removing tissue, we also evaluate the outer form. Often, what looks unpleasant is more a skin issue than a tissue issue.
· Skin redundancy
· Wrinkles
· Whether sagging is fixed in place
These factors together determine the surgical method. That’s why accessory breast surgery is not a ‘removal surgery,’ but closer to sculpting surgery.
Why does it fail if you only remove tissue?
Removing tissue reduces volume. But if stretched skin remains as-is, bulging, wrinkles, and sagging can remain. This is where surgical outcomes diverge greatly.
In reality, accessory breast surgery is not about treating ‘only the accessory breast,’ but about refining the entire axilla–chest transition structure.
Postoperative ‘natural settling process’
When the tissue is made sufficiently thin, the body settles on its own. Surfaces adhere, dead space disappears, and skin laxity decreases. We describe this as the natural settling process.
When is skin excision and lifting necessary?
Skin excision and lifting are not necessary for everyone.
We consider it only in the following cases.
· Excessive skin redundancy
· Markedly decreased skin elasticity
· Wrinkles fixed in the direction of gravity
Conversely, if the wrinkles flatten as the area becomes thinner, skin excision is not necessary.
”Accessory breast is not a lump, but a three-dimensional structure.
The key is reducing thickness and refining the boundary contour.
Accessory breast surgery is not about removing a lump—it is surgery to redesign the structure that connects the armpit and the breast.Safely, and naturally.
After surgery: care through recovery and scar management
• Scar laser: depending on individual skin healing characteristics

Er:YAG Laser

DDR Vascular Laser

Nd:YAG Laser
• Swelling & regeneration care: Capsulitis

Capsulitis

